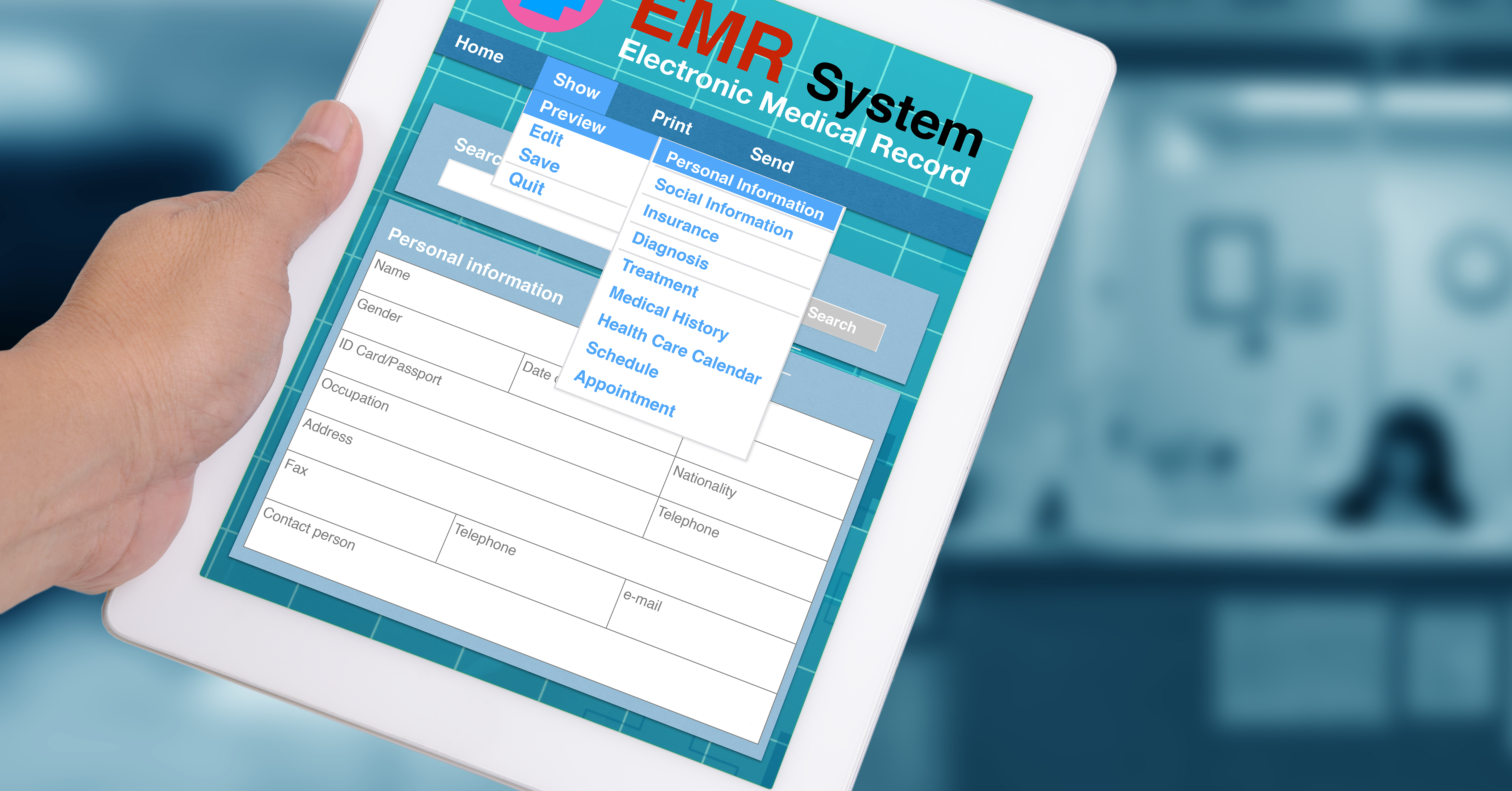
The metaSOFT EMR is the clinical core of the HMS platform — a longitudinal patient record accessible from outpatient, inpatient, emergency and any facility in the group. Every encounter, order, result and document lives in one structured record with full audit trail and role-based access control.
Every visit, test result, procedure, prescription and document in one chronological timeline, across all facilities and departments — from the patient's first visit to today.
Specialty-specific SOAP templates with ICD-10 and SNOMED coding built in; no free-text narrative that cannot be queried or audited.
Allergies, adverse reactions and high-alert medications are flagged at every prescribing point; the physician must acknowledge each alert before proceeding.
The full patient record is available to any authorised clinician in any department, any facility, on any web browser — no VPN, no desktop install.
Problem list, active medications, immunisation history and preventive care reminders are maintained in a structured, queryable view — not buried in encounter notes.
Every access, modification and disclosure is logged with user, timestamp and source. Break-the-glass emergency access is timestamped, flagged and reviewed.
The EMR is not one module among many — it is the clinical spine that every other HMS module reads from and writes to. When the pharmacy dispenses a medication, the administration appears in the patient's MAR. When the laboratory results a test, the value is immediately visible in the patient's result timeline. When the physician writes a discharge summary, it draws from structured encounter data already in the record — it does not start from a blank page.
This shared architecture means that a physician seeing a patient in the outpatient clinic has instant access to what happened during their last emergency visit, their most recent lab trends, and what medications were dispensed at inpatient discharge — without switching systems, without calling a colleague, and without waiting for a summary to be faxed.